



Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is an enveloped RNA beta coronavirus that emerged in Wuhan, China, in December of 2019 [1]. It causes the novel coronavirus disease (COVID-19), a global pandemic and has resulted in more than 175 million infections and more than 3.8 million deaths according to the World Health Organization [2].
COVID-19 vaccination drive in Korea began on the 10 February 2021 and vaccines are currently offered to frontline health and social care workers, care home residents and staff, people with chronic conditions, and older adults. As of June 13, 2021, approximately 14 million Korean populations have been inoculated the first round of vaccination. Two-thirds of those populations received AstraZeneca vaccine and the remaining one-third received Pfizer-BioNTech vaccine [3].
Whole-body [18F]F-2-fluoro-2-deoxy-d-glucose (FDG) positron emission tomography/computed tomography (PET/CT) combines functional and anatomical imaging. It has major roles in oncology for staging and post-treatment follow up of many cancers. Therefore, it is important for the reporting nuclear medicine physicians and radiologists to accurately interpret and recognize potential imaging challenges and pitfalls of false-positive FDG avidity.
Vaccinations and injections are known to cause diagnostic dilemma due to false-positive uptake locally on FDG PET/CT [4, 5]. Such dilemma can be critical for oncologic patients who might lose a chance of curative surgery due to false-positive FDG uptake at distant sites. Several case reports of lymphadenopathy post-COVID-19 vaccination have been published recently [5-8]. In this case report, we present the case of axillary and supraclavicular lymphadenopathies detected on FDG PET/CT during a staging work-up for rectosigmoid colon cancer.
Case Report
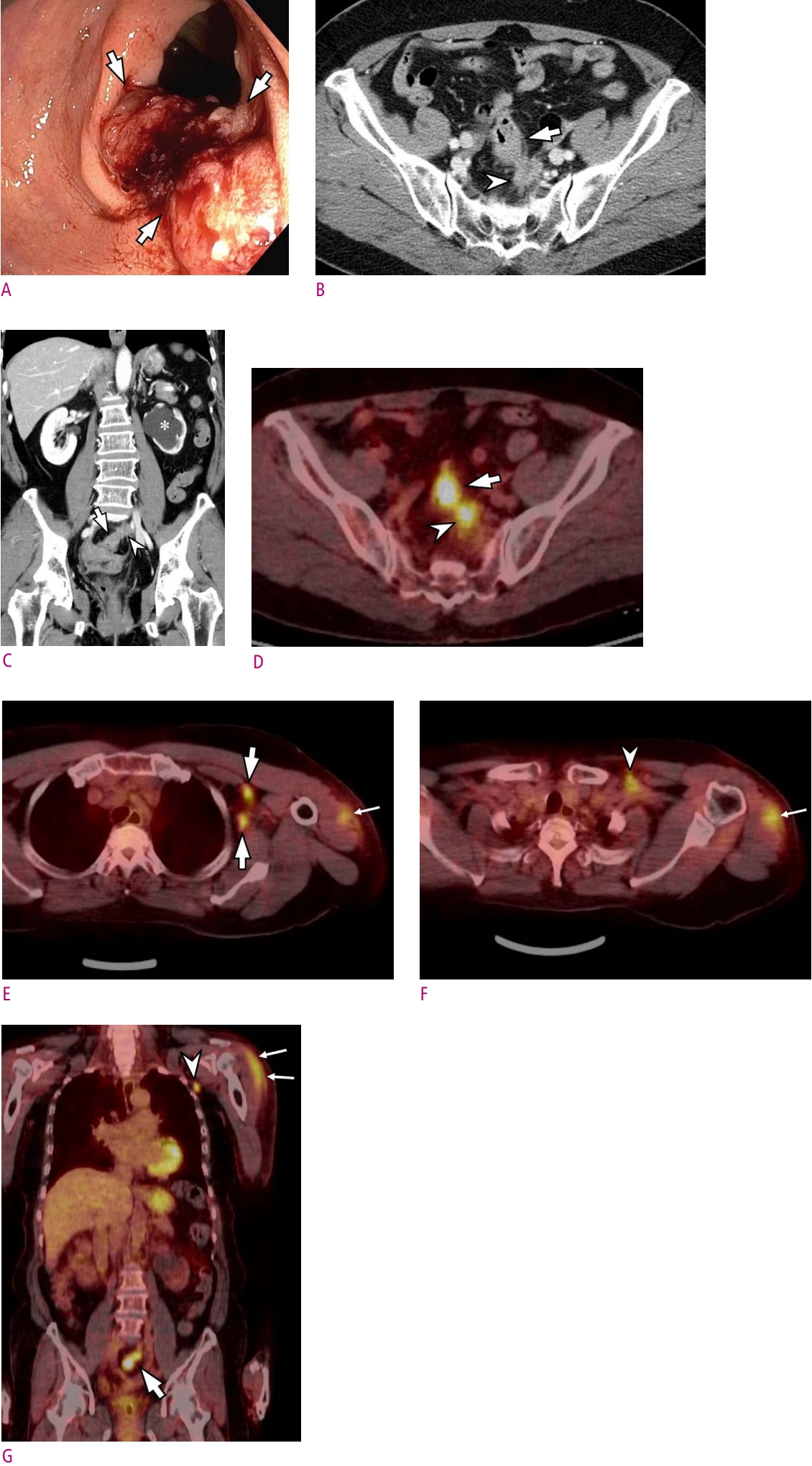
A 73-year-old woman visited our hospital for further work-up of positive stool occult blood test. Colonoscopy revealed a 5cm ulceroinfiltrative mass in the rectosigmoid junction (Fig. 1). Biopsy confirmed well-differentiated adenocarcinoma. She underwent contrast-enhanced CT and [18F] FDG PET/CT for staging work-up. On contrast-enhanced CT, there is an enhancing wall thickening in the rectosigmoid junction colon and adjacent pericolic lymph node (LN) enlargement. Left distal ureter was encased by the enlarged LN, leading to left hydronephrosis. On FDG PET/CT images, colon wall thickening and adjacent enlarged LN showed strong FDG uptake suggesting rectosigmoid junction cancer with pericolic metastatic LNs. On FDG PET/CT image at thoracic level, there were several FDG-avid LNs at left axilla area and left supraclavicular area (Fig. 1). Nuclear medicine physician initially interpreted these LNs as metastatic LNs. Therefore, palliative chemotherapy was planned. However, after a thorough image review for multi-disciplinary team (MDT) discussion by a dedicated gastrointestinal radiologist, the radiologist circumspectly noticed that there was a FDG avid lesion at left deltoid area and suggested the possibility of reactive FDG uptake after COVID-19 vaccination. After MDT conference, clinicians confirmed that the patient received COVID-19 vaccination using AstraZeneca vaccine 18 days before FDG PET/CT imaging. Therefore, management plan for the patient was changed to radical colon surgery.
Discussion
An identification of potential false-positive results on PET/CT is vital to ensure an accurate interpretation during oncologic image reporting by taking into account the clinical context because many inflammatory and reactive phenomena are known to cause false-positive avidity [9]. In our case, FDG-avid LNs at axillary and supraclavicular areas were initially interpreted as distant metastatic LNs. Therefore, clinicians including oncologists and colorectal surgeons planned palliative chemotherapy for the patient as they regarded patients as having stage IV colon cancer. However, our radiologist meticulously observed an elongated FDG uptake at left deltoid muscle and correctly diagnosed FDG-avid LNs at axillary and supraclavicular areas as reactive LNs due to COVID-19 vaccination. Subsequently, the patient did not lose a critical chance of curative resection for rectosigmoid colon cancer.
Vaccination can cause transient inflammation of LNs which demonstrates increased FDG avidity through macrophage accumulation [10]. Indeed, vaccine-related increased metabolic activity at injection site, draining LNs, systemic inflammatory response at various sites in different patterns has been reported post-vaccination for COVID-19 vaccines [5-8]. According to Schroeder DG et al., positive axillary LN uptake was observed in approximately 10% of patients on FDG PET examinations and extra-axillary LN uptake was observed only in one patient [10]. However, the previous study was performed in USA which accepted vaccines only from Pfizer, Moderna, and Yanssen pharmaceutical companies. Therefore, studies regarding FDG PET/CT after vaccination of AstraZeneca company is lacking.
An approach to the performance and interpretation of FDG PET/CT after COVID-19 vaccination should seek to provide accurate interpretations while avoiding treatment delays, additional patient anxiety, excessive follow-up imaging studies, and unnecessary biopsies. Additional imaging and tissue sampling should be cautiously suggested only when necessary. Clues towards reactive LNs include a history of recent vaccination, normal size and benign morphology of LN on CT. Further, a comparison with baseline imaging can also be helpful and if there is any doubt clinically, serial imaging, discussion in a MDT setting or tissue sampling through biopsy can be helpful in our case. Delaying scans for two to four weeks post-vaccination has been suggested; however, we feel that this may be practically difficult in oncology patients and may cause unnecessary delays.
In conclusion, we hope that this case report will alert radiologists as well as nuclear medicine physicians towards the potential pitfall of reporting LN uptake on [18F] FDG PET/CT in this current vaccination drive and provides a clear illustration of the main patterns of post-vaccine uptake which the reporting physicians or radiologists should be aware of.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






