


Introduction
Although transjugular intrahepatic portosystemic shunt (TIPS) is an effective modality for treatment of uncontrolled refractory ascites, hydrothorax or variceal bleeding, the risk for procedure-related complications is high [1]. Arteriobiliary fistula presented by hemobilia is one of major fatal complications of TIPS [2]. Most TIPS associated bleeding is primarily a complication during puncture of portal vein [2]. We are reporting a case of massive hemobilia due to hepatic arteriobiliary fistula caused by TIPS procedure.
Case Report
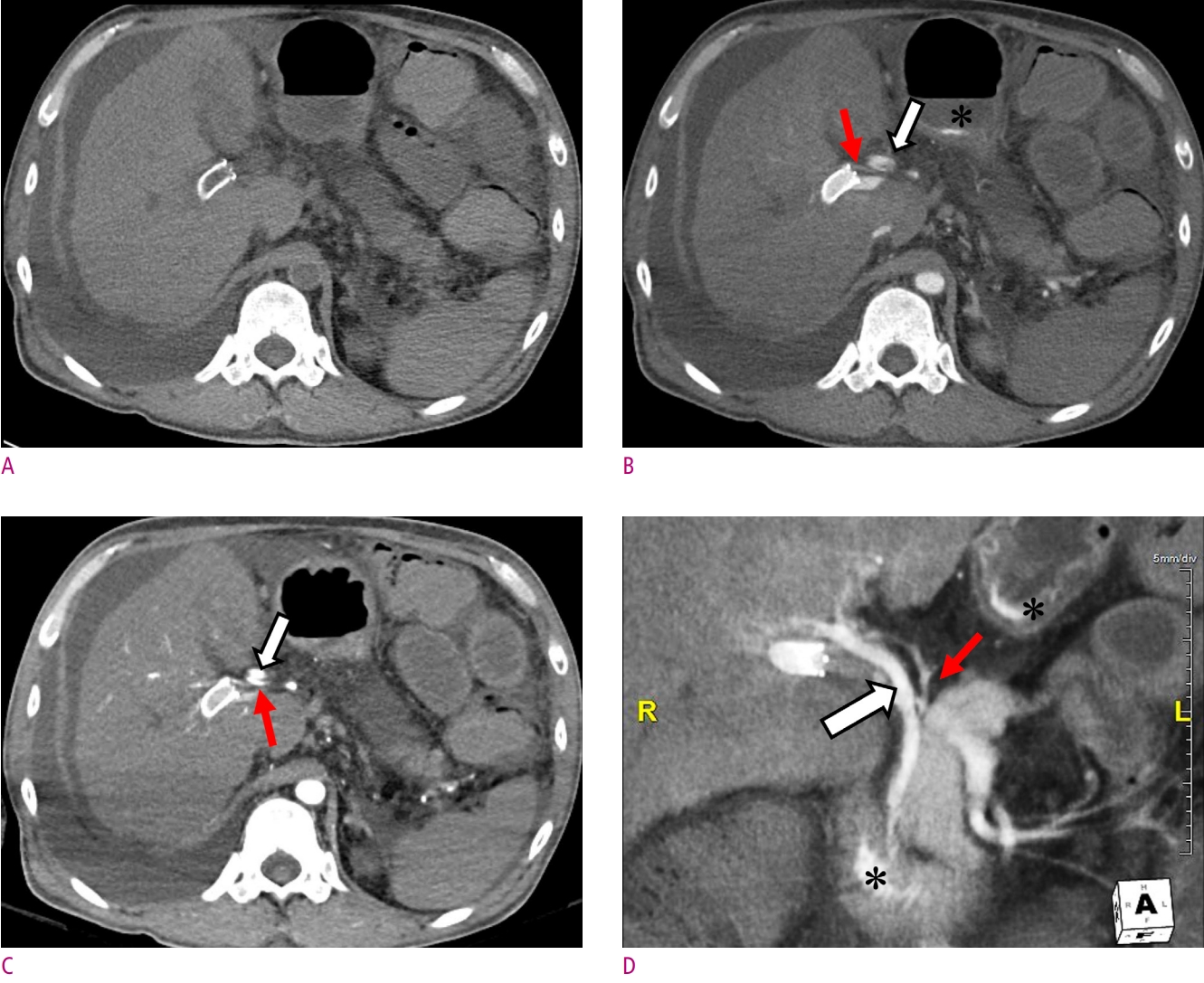
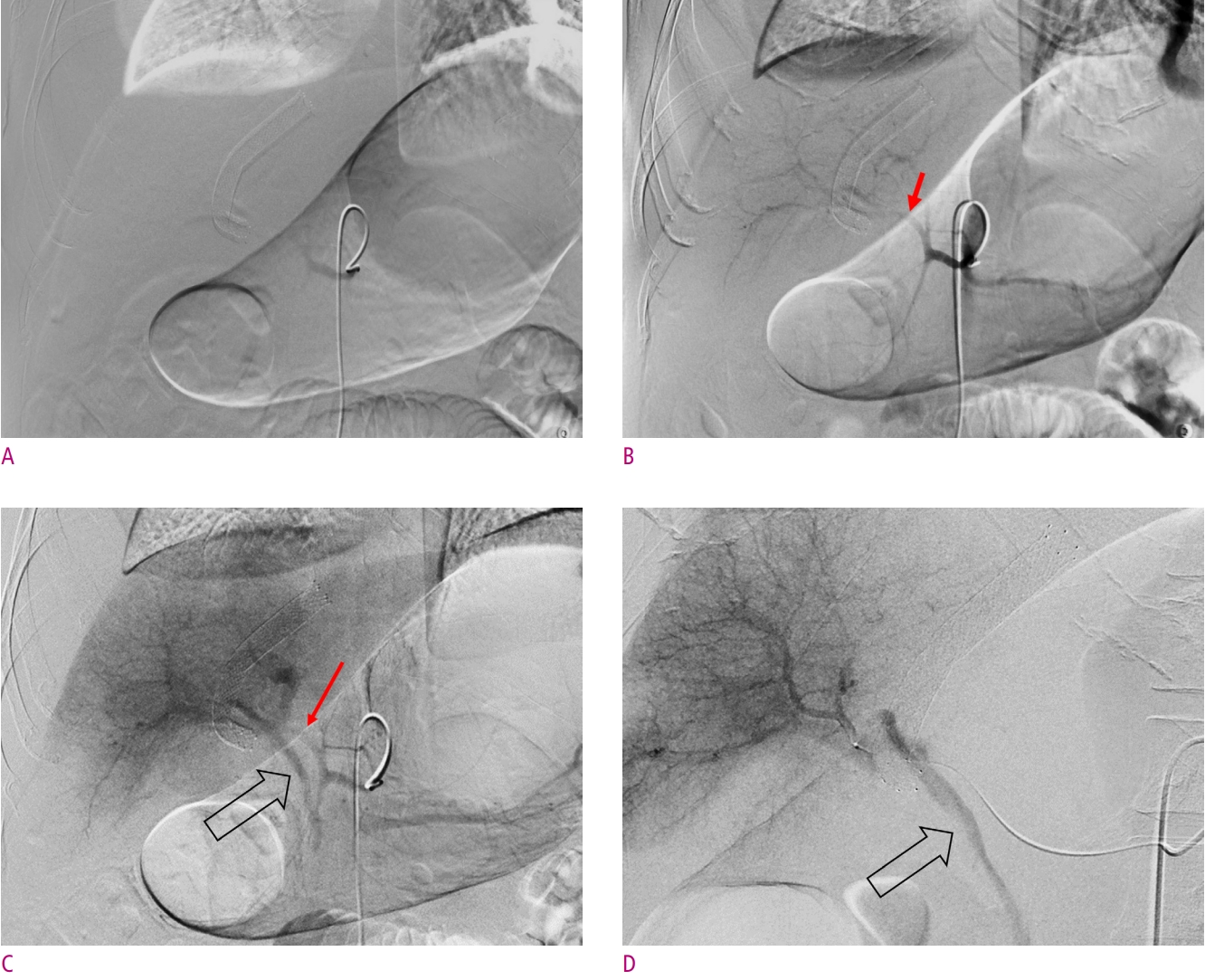
A 47-year-old man with end-stage secondary to alcoholic liver disease was admitted to our hospital for uncontrolled massive ascites, and right hydrothorax. The transjugular intrahepatic portosystemic shunt (TIPS) was planned for refractory ascites and right pleural effusion. Initial hemoglobin and platelet were 8.3 g/dL (14−17 g/dL), and 105x103/ul (130−450x103/ul), respectively. Coagulation test data were as follows: PT, 1.36 (INR, 0.88−1.13); aPTT, 39.2sec (29.1−45.1sec). Laboratory tests data were as follows: total bilirubin, 5.6 mg/dL (0.2-1.2 mg/dL); direct bilirubin, 4.1 mg/dL (0.0-0.4 mg/dL); aspartate aminotransferase, 52 U/L (8-38 U/L); alanine aminotransferase, 16 U/L (5-43 U/L); alkaline phosphatase, 102 U/L (40-130 U/L); γ-glutamyl transferase, 188 U/L (11-75 U/L); protein, 6.1 g/dL (6.4−8.1 g/dL); albumin, 2.4 g/dL (3.8−5.3 g/dL). He had a successful TIPS procedure (mean portal-systemic gradient decreased from 41 mmHg to 20 mmHg). Seven days after the TIPS, he had hematochezia, hematemesis, tachycardia, hypotension, and worsening anemia (hemoglobin dropped from 8.3 g/dL to 3.0 g/dL in 4 hours). He was in circulatory shock and was transferred to the critical care unit. He underwent CT angiography for bleeding focus evaluation. On CT angiography, the TIPS stent was patent. However, the active contrast agent leakage was noted at the distal end of stent between the right hepatic artery and the right intrahepatic bile duct. The active contrast agent leakage progressed through the common bile duct and there was reflux into the gastric antrum and the duodenum (Fig. 1). The patient immediately underwent a percutaneous angiography. Celiac trunk arteriography revealed an active contrast extravasation into the common bile duct from the right hepatic artery via the arteriobiliary fistula (Fig. 2). Subsequently, selective embolization of right hepatic artery branches was successfully performed with coils, glue and gelatin sponge. However, the patient died one day after from the disseminated intravascular coagulation.
Discussion
The TIPS is the percutaneous creation of a channel between the hepatic vein and the portal vein that is used to manage complication of portal venous hypertension [3]. Indications for TIPS include management of variceal bleeding, refractory cirrhotic ascites, hepatorenal syndrome, Budd-Chiari syndrome, and refractory hepatic hydrothorax [1, 3, 4]. As elevated portal pressure is one of the major factors contributing to the pathogenesis of ascites and hepatic hydrothorax, TIPS is a highly effective treatment option for them [5, 6]. Multiple studies have been published assessing the effectiveness of TIPS in patients with refractory ascites and technical success was achieved in 93-100% of cases, with control of ascites achieved in 27-92% and complete resolution in up to 75% of cases [1]. TIPS should be considered as a treatment option for patients who require frequent paracentesis (generally >3 in a month). In addition, TIPS has been shown to resolve hepatic hydrothorax in 60-70% of patients [5, 6].
While the primary technical success rate of TIPS placement is high, complications can occur and can drastically alter patient prognosis. Potential complications of TIPS include acute liver failure, hepatic encephalopathy, hemorrhage, biliary injury, injury to surrounding organs, TIPS thrombosis, TIPS dysfunction, and TIPS migration [1].
Serious arteriobiliary fistula complication presented as a hemobilia can occasionally occur in the early postprocedural period following TIPS placement [7]. Given the proximity of bile duct radicals to the branches of the hepatic artery and portal vein, the incidence of concurrent injury to these structures and consequent fistula formation is not unexpected. Approximately 3.8% incidence of hepatic vascular abnormalities was found following percutaneous transhepatic cholangiography [7, 8]. The frequency of clinical hemobilia is reported up to 5% after TIPS. Often hemobilia is a self-limiting phenomenon and expectant observation is a commonly used option. Clinically significant hemobilia presents with biliary colic, jaundice, and gastrointestinal bleeding, which may range from occult to massive bleeding. The initial diagnosis can be made with endoscopy [9]. CT angiography is an accurate, cost-effective tool to assess hemobilia, hematemesis, or hematochezia and can show the precise location of bleeding, thereby directing further management. Angiography with embolization is the treatment of choice for most cases of hemobilia. The goals of therapy in cases of hemobilia are to stop the bleeding and to restore bile flow. Angiography is clearly the most efficacious method for controlling intrahepatic bleeding sources, with success rates above 95% [10].
In conclusion, massive hemobilia is rare, but one of the possible complications of TIPS. A liver parenchymal puncture during a TIPS procedure may damage vascular structures such as the hepatic artery, portal vein, as well as bile duct. In cases of gastrointestinal hemorrhage after TIPS procedure, the possibility of hemobilia due to arteriobiliary fistula should be considered.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






